Incisional hernia
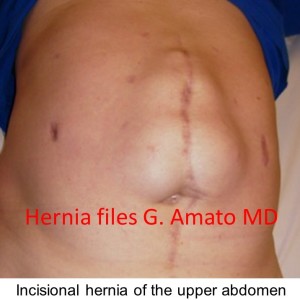 Incisional hernias are abdominal wall protrusions formed at the incision line of a previous surgery. Hernia opening can differ in size, however the hernia usually contents intestinal loops. A surgical repair to return the visceral content into the abdominal cavity, to re-establish the continuity of the abdominal wall muscles, is the procedure of choice. Complications such as incarceration or strangulation of the hernia content are rather frequent and life threatening in case of elderly patients.
Incisional hernias are abdominal wall protrusions formed at the incision line of a previous surgery. Hernia opening can differ in size, however the hernia usually contents intestinal loops. A surgical repair to return the visceral content into the abdominal cavity, to re-establish the continuity of the abdominal wall muscles, is the procedure of choice. Complications such as incarceration or strangulation of the hernia content are rather frequent and life threatening in case of elderly patients.
Incisional hernia has been well acknowledged in the scientific literature as one of the most frequent surgical procedure. Unfortunately, this kind of operation is suffering from early postoperative complications such as seroma, hematoma and wound sepsis along with other postoperative complications, including high recurrence rates of between 31% and 49% in case of non prosthetic repair.
Improvement in surgical technique, such as the use of biocompatible meshes placed to reinforce the abdominal wall, have confirmed better results with the decrease of the recurrences to below 10%.
However, the placement of prosthetic devices presents its own challenges. Site specific or small meshes have led to unacceptable failure rates which has led to a shared concept that in case of incisional hernia repair, the mesh must be wide enough to overlap the defect by a large amount.
Another issue in incisional hernia repair (both open and laparoscopic) is represented by the need for classical suture fixation. This is frequently hard to obtain, because in open repairs fixation stitches are often far away from the wound opening and difficult to be reached underneath muscles. In laparoscopic, as well as in open repair, the point mesh fixation sharply contrasts with the movements of the abdominal wall and can result in tissue tearing, bleeding or even mesh dislocation. This can prelude to recurrence
Therefore, in order to design a procedure enabling to avoid these issues, Prof. Amato has developed a modified technique based upon a newly designed implant with a special shape. This newly designed implant allows for tension free implantation method, without classic point fixation.
the freedom octomesh implant
The Octomesh implant, developed by Prof. Amato and a team of physiologists and engineers, eliminates the need for fixation (with sutures or similar). Ensures a very broad coverage of the defect, requires smaller incisions thus reducing surgical trauma. All in all, it results in a faster and easier procedure. Complication rate is very low and no recurrences are reported in a follow up of 3 years.
the technique developed by prof. amato for incisional hernia: how it works
The “tentacles” of the Octomesh implant are the key element that allows a huge step forward in terms of safety in surgical operations and clinical results.
Once positioned the mesh, the “tentacles” are tunneled with a special instrument through the fat tissue under the skin, thus ensuring the mesh an adequate holding force (friction) to keep the implant in place without sutures. This way, the mesh is perfectly anchored by 8 “tentacles”. While at same day of the procedure it takes 280 gram pull out force to dislodge one strap, 15 days later a traction force greater than 40 kg is needed to remove all the straps.
This type of fixation by friction, without sutures, (“Freexation”) is successfully used since nearly 10 years in procedures for urinary stress incontinence in women, with millions of operations performed today.
benefits for the patient
The advantages for the patient are:
- Small incision, less surgical trauma and better cosmetic results
- Broad coverage of the defect with consequent reduction of the possibility of recurrence
- Shorter operative procedure
- Low complications rate
- No recurrence, in a follow-up of 3 years
benefits for the surgeon
The advantages for the surgeon are:
- Fixation free procedure
- Easier procedure
- Faster procedure
- Broader coverage of the defect
- Standardized procedure, easy reproducibility (learning curve ca. 5 interventions)
- Great choice of implant sizes provide for a wide-ranging surgeon’s satisfaction
- Reduction of complications compared to conventional implants and no recurrences in a follow-up of 3 years
References
- Amato G. et al. Prosthetic stap system for simplified ventral hernia repair: results of a porcine experimental model. Hernia 2010;14:389-95
- Amato G. et al. A new shape of mesh to simplify and standardize the implantation procedure in ventral hernia repair. Hernia 2010;14:S-43
- Amato G. et al. Fixation free open ventral hernia repair using a new mesh with integrated placement straps. Hernia 2011;15:S21
- Amato G. et al. New mesh shape and improved implantation procedure to simplify and standardize open ventral hernia repair. A preliminary report. Hernia 2011;5:659–665
- Amato G. et al. Fixation free incisional hernia repair with a newly designed mesh with integrated bands. Hernia 2012;16 (Suppl 1): 569-572
- Amato G. et al. Fixation free incisional hernia repair in the elderly: our experience with a tentacle-shaped implant. Aging clinical experimental research. Aging Clin. Exp. Res.2017 Feb;29(Suppl 1):173-177
- Amato G. et al. Long-term results of fixation free incisional hernia repair using a tentacle shaped implant. Surg. Technol. Int. 2017 Jul 25;30:175-181.
- Amato G. et al. Long-term results of fixation-free incisional hernia repair with a tentacle-shaped implant. Hernia (2018) 22 (Suppl 1):S115
- Amato G. et al. Fixation-free incisional hernia repair with tentacle-shaped implant: The results of a long-term follow up. Hernia (2019) 23 (Suppl 2):S240